Introduction
Physical therapy in Asheville for Shoulder Issues
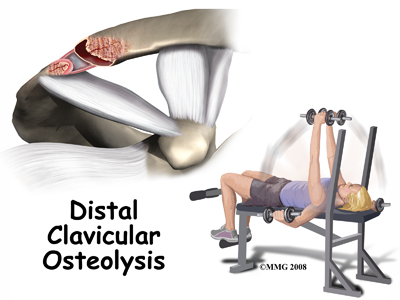 Welcome to Combined Therapy Specialties guide to Weightlifter's Shoulder (Distal Clavicular Osteolysis)
Welcome to Combined Therapy Specialties guide to Weightlifter's Shoulder (Distal Clavicular Osteolysis)
Weightlifter's shoulder is a painful deterioration of the distal end of the clavicle (collar bone). It is an overuse phenomenon that causes tiny fractures along the end of the clavicle and then a breakdown of the bone (osteolysis) occurs.
Weightlifters aren't the only ones affected; air-hammer operators, soldiers, handball players, and others can develop this problem. For this reason, it is also known as distal clavicular osteolysis (DCO). Osteolysis refers to the resorption of bone at the site of the injury.
This guide will help you understand:
- how the problem develops
- how health care professionals diagnose the condition
- what treatment options are available
- what Combined Therapy Specialties approach to rehabilitation is
#testimonialslist|kind:all|display:slider|orderby:type|filter_utags_names:Shoulder Pain|limit:15|heading:Hear from some of our patients who we treated for *Shoulder Pain*#
Anatomy
What parts of the shoulder are affected?
The shoulder is made up of three bones: the scapula (shoulder blade), the humerus (upper arm bone), and the clavicle (collarbone).
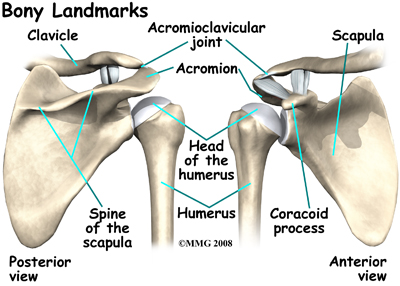
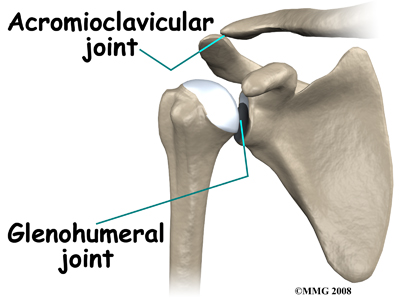
The acromioclavicular (AC) joint is affected in weightlifter’s shoulder. This is where the end of the collarbone (closest to the shoulder) attaches to the acromion. The acromion is a curved piece of bone that comes from the shoulder blade across the top of the shoulder. The clavicle and acromion meet to form the AC joint in front of the shoulder.
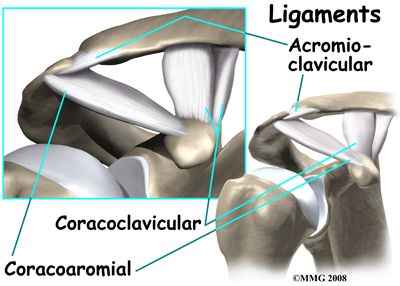
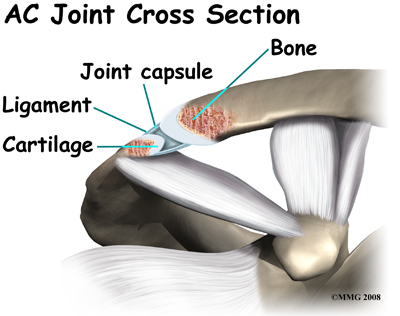
Ligaments and soft tissues hold the AC joint together and provide stability. These ligaments include the coracoclavicular ligament, superior and inferior AC ligaments, and the AC joint capsule. There is also a fibrocartilaginous disc between the clavicle and acromion to provide cushion and help transmit forces on the joint.
Related Document: A Patient's Guide to Shoulder Anatomy
Shoulder Anatomy Introduction
Causes
What causes this condition?
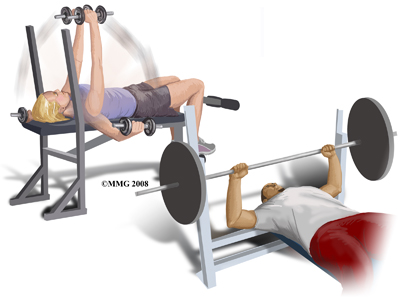 Repetitive trauma or stress from training and lifting causes tiny fractures of the distal end of the clavicle bone. Excessive traction on the AC joint from bench presses or chest fly exercises occurs when the elbows drop below or behind the body. This places the shoulders in a position of excess extension. As the bone does not have a chance to heal before the next training session begins, the bone actually starts to dissolve.
Repetitive trauma or stress from training and lifting causes tiny fractures of the distal end of the clavicle bone. Excessive traction on the AC joint from bench presses or chest fly exercises occurs when the elbows drop below or behind the body. This places the shoulders in a position of excess extension. As the bone does not have a chance to heal before the next training session begins, the bone actually starts to dissolve.
Some people affected by weightlifters shoulder may have a history of an acute injury of the AC joint but the condition can occur without any known previous trauma. In most cases, there is repetitive stress to the affected upper extremity. As mentioned above, weight training, intensive lifting, and operating an air hammer are examples activities that can lead to acute distal clavicular osteolysis.
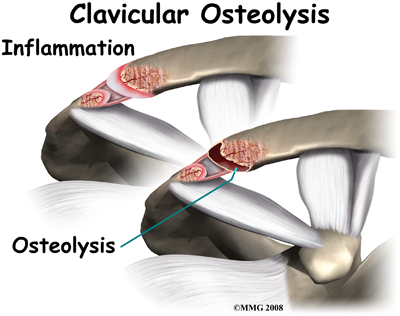 In studying this injury, there is evidence that the body tries to heal the fractured bone but the bone dissolves or is resorbed by the body instead. A network of blood vessels forms in the area during the attempted healing process. Chronic inflammation with scar tissue called fibrosis is commonly found when tissue from the area is examined under a microscope.
In studying this injury, there is evidence that the body tries to heal the fractured bone but the bone dissolves or is resorbed by the body instead. A network of blood vessels forms in the area during the attempted healing process. Chronic inflammation with scar tissue called fibrosis is commonly found when tissue from the area is examined under a microscope.
Part of the breakdown process of the joint is from the fact that the synovial lining, which lines most joints, starts to overproduce itself during this injury and invasion of the underlying bone begins. Degenerative joint disease occurs as an end-result of the pathologic process.
Symptoms
What are the symptoms?
Symptoms include an aching pain in the front of the shoulder at the AC joint. Pressing on the AC joint causes increased pain and tenderness. There is often weakness associated with the degenerative bone changes. For the weightlifter, symptoms are the most severe the night after a weightlifting competition or program. Other symptoms include pain when you are moving the arm across the body, and the pain increases with weight training involving the upper extremities (arms). Activities such as push-ups, bench presses, power clean exercises, dips on the parallel bars, and throwing motions make the symptoms worse. Lying on the affected side can disrupt sleep.
Diagnosis
How will my health care professional diagnose this condition?
The history and physical examination are probably the most important tools health care professionals use to diagnose any condition. Your health care professional may move and feel your sore joint. This may hurt a bit, but it is very important that they understand exactly where your joint hurts and what movements cause you pain.
The definitive diagnosis is made using X-rays, bone scans, and a steroid injection. CT-guided injection is actually a diagnostic tool and a treatment. Pain relief with steroid injection into the AC joint confirms that the pain is coming from the AC joint.
Treatment
What treatment options are available?
Nonsurgical Treatment
Treatment begins with conservative (non-operative) care. This may include rest and/or changes in weight-training activities and techniques. Avoiding over-training and smoking are two very effective ways to prevent this condition. Over-training adds too much stress to the bone, which can contribute to rapid bone breakdown. Smoking decreases the amount of oxygen available to the bones and tissues and thus creates a less resilient tissue. If you do develop weightlifters shoulder, take quick steps to modify your weightlifting techniques and avoid over-training.
One of our physical therapists at Combined Therapy Specialties can help you with advice for activity modification and specific strength training tips for this problem. For example, if you narrow your hand spacing on the barbells this takes the stress off the distal clavicle. Stopping your bench press two inches above the chest also decreases the stress on the distal clavicle. Some lifters place a two-inch folded towel on the chest as a reminder of when to stop.
The power clean or power jerk can also be modified. Don't rack the bar (lift the bar and let it rest on the clavicles or deltoids.) Start with the elbows even with, or above your shoulders and lift. This eliminates the power pull. If you do develop weightlifters shoulder then certain activities such as bench press, dips, and push-ups should be avoided for a while to allow healing. Applying ice massage and taking ibuprofen after each workout or exercise session can help.
If you work directly with a personal trainer they should also be able to provide tips for proper technique during your actual session to avoid this injury, along with other common weight lifting injuries.
Athletes must be careful to follow all recommendations for program modifications. There is a tendency to work through the pain and not really modify the program at all.
In addition to modifying your weightlifting technique, any muscular imbalances around your shoulder should be addressed. Your physical therapist at Combined Therapy Specialties will assess the strength of your shoulder, chest and back muscles and determine if any areas are not strong enough or other areas are too strong in comparison to the rest.
Weightlifters are prone to have stronger chest and shoulder muscles than those of the back and posterior shoulder. This imbalance can also contribute to the pressure on the distal clavicle, and the development and lingering pain of weightlifters shoulder. Your physical therapist will prescribe exercises for you that address any imbalance that is present. Often the exercises we prescribe to correct the imbalance will be similar to the ones that you have been doing at the gym already, and can be done with barbells or light weights, but the ratio of exercises that are done for your chest and anterior shoulder is often much less than what we will prescribe for your back and posterior shoulder. Proper technique is also of utmost importance so we will ensure you use good technique before using weights that are heavy.
Imbalances around the shoulder can also occur because of tissues that are too tight.
Your physical therapist will also assess which muscles you should be stretching in your particular case to address any imbalances. Again, weightlifters have a tendency to be tight around the chest and anterior shoulder, but these areas will be individually assessed by your physical therapist to decide whether this is the case for you in particular.
In addition to addressing any strength and range of motion imbalances around your shoulder, rehabilitating the shoulder from this injury requires exercises that address your shoulder proprioception. Shoulder proprioception is the unconscious ability for you to know where your shoulder is in space during everyday, as well as sporting activities.
Gaining adequate shoulder proprioception, especially of the shoulder blade, is a extremely important component of any shoulder rehabilitation program because the shoulder is a very mobile joint that easily becomes pinched or impinged if it is not moving well. This impingement is even greater when under load, such as lifting weights.
Your physical therapist will spend time teaching you proper shoulder proprioception and prescribe specific exercises for this, such as gentle rowing with a light band, or overhead reaching and pulling while you focus on the position of your shoulder blade.
At Combined Therapy Specialties we also encourage you to maintain your body’s overall fitness level even if you have had to take a break from your regular weightlifting or substantially decrease the amount you are doing. A stationary cycle, elliptical, or step machine can all be useful ways to maintain your cardiovascular health while you recover from your injury. If you are a runner, you may be able to continue running as long as the pumping action of the arms does not induce your shoulder pain.
With conservative care and the proper rehabilitation routine outlined by one of our physical therapists at Combined Therapy Specialties, you will likely feel a lessening of painful symptoms until you are pain free. As you improve, your physical therapist will help you gradually resume all activities without bringing back the problem.
If the pain does not resolve with conservative care, or you are not able to resume your normal activities, surgical intervention, which removes, or ‘resects’ a portion of the end of the clavicle bone may be required. In cases such as these, your physical therapist will refer you on to seek the opinion of an Orthopaedic Surgeon.
Interestingly, some athletes who progress through the pain without activity modification, may, in a way, perform surgery on themselves. In this form of self-surgery, as the injury progresses the clavicle will resect on its own as the bone breaks down and breaks off. Unfortunately, there will still be an inflammatory response with increased symptoms that still sets you back in your program. In addition, if the body doesn’t resorb the broken off bone, surgery may be required anyways to extract it. It is our recommendation at Combined Therapy Specialties that a period of activity modification in addition to an appropriate rehabilitation program is adhered to.
Combined Therapy Specialties provides services for physical therapy in Asheville.
Surgery
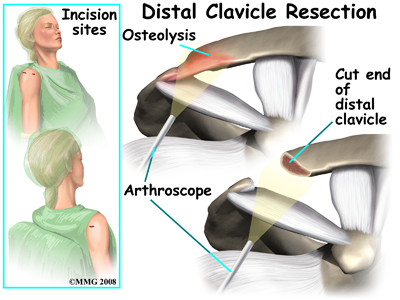
Surgery may be needed for those athletes who do not improve with conservative care or who are unwilling to change their training or performance routine. The surgeon removes the end of the clavicle. This is called a distal clavicle resection. The procedure can be done with an open incision or through tiny athroscopic puncture holes.
During the surgical procedure repair of any torn soft tissue in the area is also completed. Some surgeons transfer the coracoacromial ligament over the end of the bone that has been cut which helps stabilize the joint for a quick return-to-sport. This transfer often makes power lifting more comfortable for many athletes.
Post Surgical Rehabilitation
We recommend that you follow up at Combined Therapy Specialties to see one of our physical therapists immediately after your surgery. We will ensure that the shoulder is moving well and that your pain is under control. If it needed, we may use some electrical modalities such as ultrasound or interferential current or may do some massage to ease any residual surgical pain you may have. Your physical therapist will then prescribe some range of motion and gentle strengthening exercises to ease the shoulder back into full range and bearing some load. We will also focus on the proprioception of your shoulder joint (as outlined under non-surgical rehabilitation) so that you can return to weightlifting without any complications and avoid other injuries in the future. Fortunately, rehabilitation after surgery for weightlifters shoulder goes very quickly and if you are doing well even after the first time you see us, you may be able to start back carefully and gently at light weight lifting. Many experienced weightlifters are able to return back to some of their weight training routine as early as three days after surgery. A graduated return to full weights over a couple of weeks is the preferred schedule, especially if competition is not imminent.
Maintaining the rest of your body’s fitness during recovery is highly recommended. Cardiovascular work on a stationary cycle or step machine can be done immediately, and weights for the lower extremities can continue as long as you have a training buddy to help you prepare your weight racks so your surgical arm does not have to lift excessive weight.
Fortunately with surgery, pain is relieved in the majority of patients. Weightlifters are pleased that without the pain, they can quickly get back to their pre-operative level of lifting. In fact, some even report exceeding their training weight once the pain is gone.
Likewise, there are reports of manual laborers quickly returning to full work duties.
Patients should be warned, however, that there could be some problems. Abnormal motion prior to the surgery of the acromioclavicular joint can lead to a poor result. In such cases, pain is not relieved. There can be muscle injury, prolonged bleeding, infection, and fracture of the clavicle during the procedure. It should also be mentioned that smokers are at greater risk of poor wound healing and failed surgery.
Generally recovery from surgery for weight lifter’s shoulder goes extremely well and very quicky. If, however, your rehabilitation is not progressing as well as your physical therapist at Combined Therapy Specialties expects it to, we will ask you to follow up again with your surgeon to confirm that there are no complications from the surgery that are impeding your rehabilitation.
Portions of this document copyright MMG, LLC
Combined Therapy Specialties provides services for physical therapy in Asheville.








